Gastroesophageal Reflux Disease
Gastroesophageal Reflux Disease
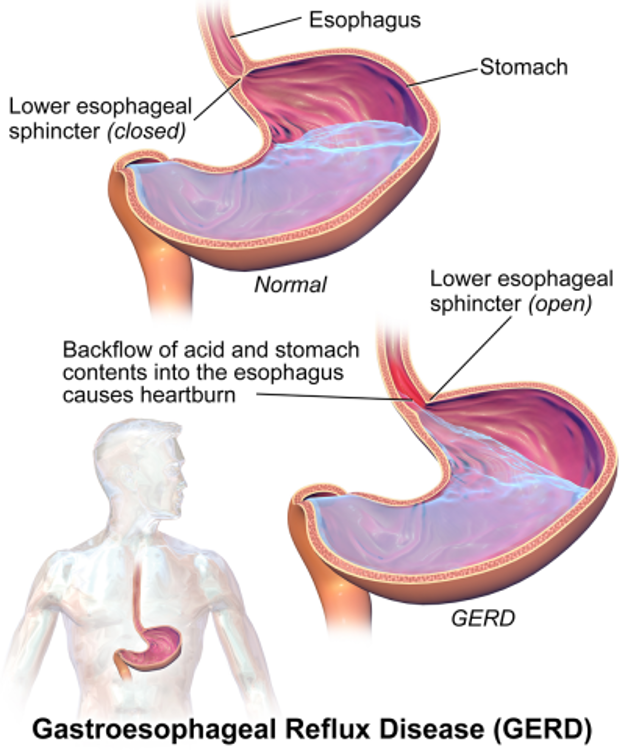
The esophagus (ĕ-sof´ah-gus) is the hollow, muscular tube that moves food and liquid from your mouth to your stomach. A ring of muscle fibers at the bottom of the esophagus keeps the stomach contents from moving backward.
In some people, the muscles don’t work properly so the contents of their stomach flow backward into their esophagus and causes problems, such as heartburn or reflux. If this happens more than twice per week, you may have gastroesophageal reflux disease (GERD).
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) estimates that one in 20 people has GERD. The disease can affect anyone, including infants and children, but it is most likely to occur among those who are overweight, pregnant, smoke, or take certain medicines.
Causes Of GERD
It is unclear why GERD occurs but alcohol and certain foods, such as citrus, chocolate, fried foods, and spicy foods, have been associated with reflux events.
Symptoms Of GERD
- Heartburn
- Reflux
- Dyspepsia
- Shortness Of Breath
Symptoms of GERD include:
- A burning sensation in the chest (heartburn)
- Backing up of stomach acids (reflux) with a sour or bitter taste in your mouth
- Stomach discomfort (dyspepsia) with nausea or bloating after eating
- Shortness of breath or a chronic cough associated with heartburn
It also can cause problems with swallowing because your esophagus narrows (esophageal stricture), breathing problems because of stomach acid getting into your lungs (aspiration), or Barrett’s esophagus.
If you have a history of heartburn or acid reflux, talk to your doctor because prolonged symptoms increase your risk of developing inflammation of the esophagus (esophagitis).
If you have symptoms of GERD, your doctor may first recommend over-the-counter antacids and lifestyle changes, such as losing weight, eating smaller meals, avoiding certain foods, and remaining upright for 3 hours after a meal.
Diagnosis And Treatment Options
Prescription medications may be the next step, but often aren’t recommended for long periods due to potential side effects.
If your symptoms do not improve, you may need to undergo diagnostic tests, such as a barium swallow x-ray, CT scan, upper endoscopy, esophageal function testing (manometry) or an ambulatory pH monitoring examination.
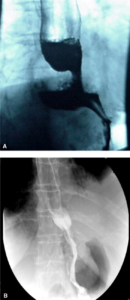
Barium swallow before (A) and after (B) surgery
If GERD is diagnosed and medication and lifestyle changes do not work, antireflux surgery may be a treatment option.
Surgical or interventional procedures may be considered for patients who do not want to take lifelong medications or are concerned about side effects like osteoporosis.
Antireflux Surgery
Patients with reflux often have a hiatal hernia (the stomach has pushed up through the diaphragm and into the chest), which can be repaired laparoscopically or robotically during antireflux surgery, although a larger incision through the chest or abdomen may be recommended, especially if your hernia is larger, you are overweight, or your esophagus is relatively short due to scarring.
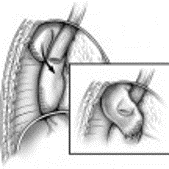
Options for antireflux surgery include Nissen fundoplication, LINX magnetic sphincter augmentation and transoral incisionless fundoplication (TIF).
During Nissen fundoplication surgery, the upper part of the stomach (fundus) is wrapped around the esophagus to reinforce the valve between the esophagus and stomach, making acid less likely to back up into the esophagus. The procedure usually is done using a minimally invasive (laparoscopic) approach through small incisions in the abdomen.
LINX magnetic sphincter augmentation consists of an implantable magnetic band surgically placed around the lower esophagus.
Transoral incisionless fundoplication (TIF) is an endoscopic procedure performed by a surgeon or highly specialized gastroenterologist. If the patient has a hiatal hernia a surgeon will need to reduce and repair the hernia, usually performed with minimally invasive robotic surgery, in combination with TIF.


You will need to adjust your eating after the surgery. Immediately after surgery, you should eat only soft foods.
Recovery
If the minimally invasive method is used, you likely will be in the hospital for 2 to 3 days and may be able to return to your normal routine in 2 to 3 weeks. With open surgery, patients stay in the hospital for 5 to 7 days with a 6- to 7-week recovery. With a hiatal hernia, it is important to avoid heavy lifting for at least 6 to 8 weeks to help prevent a recurrent hernia.
Eventually you can return to a more normal diet but should be sure to chew more thoroughly and eat more slowly.
Occasionally, patients can have diarrhea (dumping syndrome) after eating certain foods, such as sweets, which can be improved by changing your diet.
After a Nissen fundoplication, it is also important to avoid large pills and foods that cause gas, such as carbonated beverages, because the reinforced valve can make it more difficult to burp or vomit.