Atrial Fibrillation
Atrial Fibrillation (Afib)
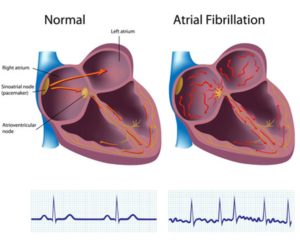
What Is Atrial Fibrillation? Atrial fibrillation, or Afib, is the most common type of irregular heartbeat (arrhythmia).
Normally, the upper chambers of your heart (the atria) squeeze first, followed by the bottom part (the ventricles). This contracting and relaxing creates the familiar “lub-dub” beat. The movement pushes blood from the upper heart chambers to the lower ones and out to your body. When you have Afib, the electrical signals that control your heartbeat are out of sync. Instead of working together, the atria quiver or fibrillate; your heart races rather than beats. With Afib, your heart can’t pump blood through its chambers and out to your body as well as it should.
According to the American Heart Association, approximately 2.7 million Americans are living with Afib. It is common in people age 60 and older and can lead to blood clots, stroke, heart failure, and other heart-related complications. Untreated Afib doubles the risk of heart-related death and is associated with a 5-fold increased risk for stroke.
Types Of Afib
The different types of Afib include:
Paroxysmal Afib is when the heart returns to a normal rhythm on its own, or with intervention, within 7 days of when the condition started. This Afib may last for seconds or up to a week before the heart returns to its normal rhythm. Symptoms, which can be mild or severe, are unpredictable and may occur a few times a year or every day. Paroxysmal Afib does not usually require treatment, but often can turn into a permanent form of Afib.
Persistent Afib usually lasts longer than a week. While it may stop on its own, this type of Afib may require medicine or treatment (cardioversion) to help the heart return to normal rhythm.
Long-standing persistent Afib is when your Afib has lasted at least a year without interruption. This Afib can be the most challenging to treat. Medications to maintain a normal heart rate or rhythm are often ineffective. More invasive treatments may be needed to restore your normal heart rhythm.
Permanent (chronic) Afib occurs when the condition lasts indefinitely and cannot be corrected by treatments. This means that your heart is in a state of Afib all the time and that you and your health care team have made a decision not to pursue interventions. However, you may need long-term medication to control your heart rate and lower your risk of stroke.
Causes And Symptoms
- Heart Attacks
- An Overactive Thyroid Gland
- Long-term Consumption Of Stimulants
- Sick Sinus Syndrome
- Lung Disease
- Viral Infections
Causes
Sometimes the cause of Afib is unknown. Other times, conditions such as uncontrolled high blood pressure or coronary artery disease may damage the heart’s electrical system. Afib also is the most common complication after heart surgery. In addition, Afib is closely linked with age. The older you get, the higher your risk is of developing it.
Other possible causes of Afib include:
- Heart attacks
- Abnormal heart valves
- Congenital heart defects
- An overactive thyroid gland (hyperthyroidism)
- Regular, excessive, long-term consumption of stimulants, such as medications, caffeine, tobacco, or alcohol
- Sick sinus syndrome — improper functioning of the heart’s natural pacemaker
- Lung disease, such as chronic obstructive pulmonary disease (COPD) or emphysema, or a blood clot in your lung (pulmonary embolism)
- Viral infections
- Obesity, diabetes, and metabolic syndrome
- Stress due to pneumonia, surgery, or other illnesses
- Sleep apnea
Symptoms
What does Afib feel like?
You might feel a flutter or quiver in your chest when your heart beats. Your heart also might race or beat faster than usual. The feeling often lasts for a few minutes. Sometimes your heart will skip a beat. However, the symptoms of Afib are different for each person, depending on factors such as age and cause. Many people with Afib feel no symptoms at all, while others may feel:
- Tired or lack of energy
- Pulse that is faster than normal or changing between fast and slow and feels irregular
- Short of breath
- Heart palpitations (feeling like the heart is racing, pounding, or fluttering)
- Dizziness, lightheaded, or faint
- Pain or pressure in the chest
Some of these symptoms, such as shortness of breath and chest pain, can mimic those of a heart attack. If you aren’t sure whether you have Afib or you’re having a heart attack, call your doctor or 911.
Diagnosis And Treatment Options
Diagnosis
If your doctor thinks you have Afib, the first thing he/she probably will do is listen to your heartbeat’s rate and rhythm and take your pulse and blood pressure. The doctor also will ask detailed questions about any symptoms, health habits and problems, and family medical history. Sometimes your primary care or family doctor will be the one who diagnoses Afib. But your doctor also may refer you to a:
- Cardiologist: a doctor who specializes in heart diseases and conditions
- Electrophysiologist: a cardiologist who specializes in arrhythmias
The doctor may order several tests to diagnose your condition, including:
- Electrocardiogram (EKG) is a simple, painless test that records the heart’s electrical activity. It’s the most useful test for diagnosing Afib.
- Holter monitor records the heart’s electrical activity for a full 24- or 48-hour period. You wear this portable EKG device while you do normal daily activities.
- Event recorder is a portable EKG device intended to monitor your heart activity over a few weeks to a few months. You activate it only when you experience symptoms of a fast heart rate.
- Echocardiogram (echo) uses sound waves to create a moving picture of your heart. The test shows the size and shape of your heart and how well your heart chambers and valves are working.
- Transesophageal echocardiography (TEE) uses sound waves to take pictures of your heart through the esophagus. The heart’s upper chambers are deep in your chest and can be seen much better using TEE.
- Stress test puts extra stress on your heart to see how it responds to working hard and beating fast. You’ll be hooked up to an EKG during the test, and the technician will watch your heart rate and blood pressure.
- Blood tests can indicate what may be causing your Afib. Blood tests check for infection, thyroid and kidney problems, and signs of a heart attack.
- Chest X-ray will not show Afib, but it can show complications, such as fluid buildup in the lungs and an enlarged heart.
Treatment Options
Treatment for Afib depends on how often you have symptoms, how severe they are, and whether you already have heart disease. General treatment options include medications, medical procedures, and lifestyle changes. Your doctor will help you decide which treatment is right for you.
Medications
Medications for Afib can help prevent clots and strokes, slow your heart rate, and control your heart rhythm.
Blood thinners to prevent clots and stroke
Because Afib prevents normal blood flow, blood can pool in the atria and form clots. If a clot travels to your brain, it could cause a stroke. Blood-thinning medicines, such as warfarin, aspirin, and heparin, help prevent blood clots and stroke. In fact, they can lower your chances of a stroke by 50% to 70%. However, they also can raise your chances of bleeding, so you might have to cut back on some activities that can lead to injuries.
Some medications and vitamins change the way blood thinners work in your body, so you can expect to see your doctor for a blood test every month to make sure the medication is working and you’re on the right dose.
Beta blockers
Beta blockers don’t fix the abnormal heart rhythm, but they can help you feel better by slowing your heart rate so that your heart can pump better.
Calcium channel blockers
Calcium channel blockers relax blood vessels in your heart and slow your heart rate.
Digoxin
Digoxin works on your heart’s electrical system to slow the rate that signals move from the atria to the ventricles.
Channel blockers
The most common way to treat atrial fibrillation is with medications that control the heart rhythm by slowing the electrical signals through your heart. This type of treatment is called cardioversion with drugs or chemical cardioversion. These medications—sodium and potassium channel blockers—slow the electrical signals to bring your heartbeat into what’s called a normal sinus rhythm. Sodium channel blockers slow your heart’s ability to conduct electricity, while potassium channel blockers slow the electrical signals that cause Afib.
Your doctor will watch your heart rhythm during treatment to see how well the medicine is working, so it’s likely that you’ll receive this type of treatment in a hospital or at the doctor’s office.
Catheter Ablation
Catheter ablation is a nonsurgical treatment for Afib that works by scarring tissue in your heart to disrupt faulty electrical signals. The doctor threads a long, flexible, thin tube (catheter) into a blood vessel in your groin, shoulder, or neck. Using ultrasound, he/she will guide the catheter into your heart. The end of the catheter is used to apply heat or extreme cold to certain parts of the heart muscle, causing tiny scars that disrupt or eliminate the erratic electrical signals in your heart.
Some people leave the hospital the same day, or you may have to stay in the hospital overnight after the ablation.
Maze Procedure
The types of maze surgery include:
Open heart maze procedure: If you have Afib and are undergoing other necessary heart surgery, such as coronary artery bypass surgery or heart valve repair, your surgeon may perform a maze procedure during open-heart surgery. This is the most common type of maze procedure. The surgeon creates a path or maze of scar tissue in the upper chambers of your heart, using a scalpel or an ablation device. The scars make a path for electricity in your heart to follow, allowing your heartbeat to become normal.
Minimally invasive maze surgery: Also known as the “mini maze,” this procedure allows the surgeon to correct the electrical irregularity in the upper chambers of your heart without performing open heart surgery. The surgeon reaches your heart through small incisions called keyholes. Using a tiny video camera to help see your heart, he/she will use heat or extreme cold to form scar tissue on your heart. The scar tissue prevents the abnormal electrical impulses from affecting the rest of the heart. With the minimally invasive maze procedure, you may experience fewer complications and a shorter hospital stay than with traditional open surgery.
Insert Convergent Article
https://www.atricure.com/download-asset-file/8520
Pacemaker
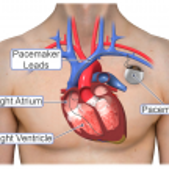
If you have Afib with a slow heartbeat, your doctor may suggest placing a pacemaker in your chest. A pacemaker is a small device that monitors your heartbeat and sends out a signal to stimulate your heart if it’s beating too slowly.
The device consists of a small box (generator) that holds a battery and tiny computer. Thin wires called leads connect the pacemaker to your heart. Impulses flow through the leads to keep your heart in rhythm.
Having a pacemaker placed is a minor procedure. Your doctor will insert a needle into a large vein near your shoulder, guiding the leads into your heart. The pacemaker then goes into your chest through a small cut. Once it’s in place, your doctor tests it to make sure it works.
Living With Afib
Life with Afib has its challenges, but with the right treatment and some lifestyle changes, you can live a normal, active life. It’s important to recognize, though, that living with Afib can affect many different aspects of your life, including your stamina, relationships, and emotional health. Taking an active role in your care can help you feel better and more in control.
A healthy lifestyle is especially important if you have Afib. You should be particularly mindful about eating a heart-healthy, balanced diet that is low in fat and salt, while also limiting your intake of alcohol and other stimulants such as strong tea or coffee and caffeine-based drinks. If you smoke, you should stop. Nicotine can make Afib worse. Smoking also damages your blood vessels and raises your chances for heart disease and heart attack.
Moving your body also can make a difference. Light to moderate exercises, such as walking, swimming, and riding a bike, are good options, but talk with your health care team about what exercise routine is best for you. Staying active will help you control your weight, improve your sleep, and make your heart stronger. In addition, exercising may help minimize worry and anxiety that can make Afib worse due to faster heart rates. If your stress feels overwhelming, reach out to your doctor, family, and friends. You also may want to consider joining an Afib support group or talking with a professional counselor.