Thoracic Aortic Aneurysm
Thoracic Aortic Aneurysm
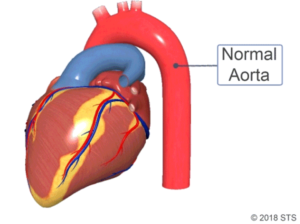
The aorta is the main artery that carries blood out of the heart to the rest of the body. Blood flows out of the heart and into the aorta through the aortic valve. Roughly the diameter of a garden hose, the artery extends from your heart down through your chest and into your abdomen, where it divides into a blood vessel that supplies each leg.
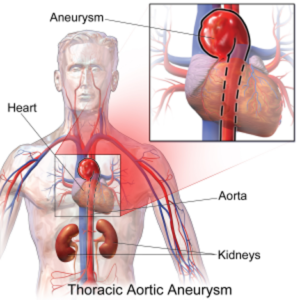
An aneurysm is a weakening in the wall of an artery, which causes it to “balloon” or expand in size. Although an aneurysm can develop anywhere along your aorta, most occur in the section running through your abdomen (abdominal aneurysms). Others occur in the section that runs through your chest (thoracic aneurysms) and above the diaphragm.
According to the US Centers for Disease Control and Prevention, aortic aneurysms were reported as the primary cause of 9,863 deaths in the US in 2014, but the actual number is likely much higher.
Aneurysms are often found incidentally during evaluation of other problems. Since they commonly cause no pain or discomfort, aneurysms can silently enlarge for long periods of time without being identified. When the aneurysm gets too large, it can cause pressure on a neighboring organ, or the wall of the blood vessel can split or tear (aortic dissection/dissecting aortic aneurysm) or even “burst” under the pressure (aortic rupture/ruptured aortic aneurysm).
Causes Of Thoracic Aortic Aneurysms
Many factors can contribute to the development of an aortic aneurysm. Some of the most common conditions associated with aneurysm formation are:
- High blood pressure (hypertension)
- Smoking, leading to injury of the wall of the aorta
- Hardening of the arteries (atherosclerosis) where fat, cholesterol, and other substances (plaque) clog the arteries
- Changes in your aorta due to advanced age
- Inflammation of your aorta
- Injury from falls or motor vehicle accidents
- Untreated infection such as syphilis or salmonella
- Congenital or genetic causes of weakness of the artery wall (present from birth), such as bicuspid aortic valve, Marfan or Ehlers-Danlos syndrome
In some cases, aneurysms run in families and are classified as “familial”, so several members of extended families may be affected by aneurysms in different locations.
Symptoms Of Thoracic Aortic Aneurysms
Thoracic aortic aneurysms often do not cause any symptoms and they usually develop slowly over time. However, if the aneurysm is big enough to put pressure on a surrounding structure, you may experience symptoms such as:
- Hoarseness
- Trouble swallowing
- Swelling in your neck
- Pain in your chest or upper back
- Nausea and vomiting
- Rapid heart rate (tachycardia)
Because thoracic aortic aneurysms usually develop slowly and do not cause many symptoms, they can be hard for doctors to detect and diagnose.
Diagnosis And Treatment Options
Because thoracic aortic aneurysms usually develop slowly and do not cause many symptoms, they can be hard for doctors to detect and diagnose. Unless the aneurysm has expanded significantly or ruptured, a physical exam by your doctor likely will be normal.
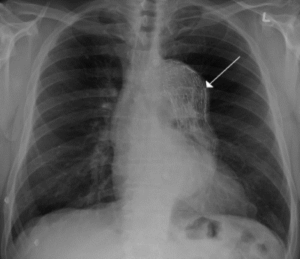
Undergoing imaging tests for other symptoms or conditions is often how thoracic aortic aneurysms are detected. These tests can include a chest x-ray, echocardiogram (ultrasound of the heart and part of the aorta), a computed tomography (CT) scan, or a magnetic resonance imaging (MRI). A CT scan or MRI show the size of the aorta and the exact location of the aneurysm.
Most aneurysms are incidental findings that do not require surgery initially and can be managed with tight blood pressure control. It is important to continue to follow up with your surgeon to make sure the aneurysm does not increase in size (diameter). Significant growth of the aneurysm (increase by 0.5 to 1 cm in a year), is a sign that the aneurysm should be repaired, no matter the overall size. When the aneurysm is slowly enlarging over many years, surgeons have traditionally used 5.5 cm as the cut off for surgical repair. The risk of a complication such as dissection or rupture increases significantly after an aneurysm reaches 6 cm, so it is best to undergo treatment before reaching this threshold.
However, your height also helps determine when to undergo surgery, as a shorter person may have a smaller aorta and will need surgery when the size of the aneurysm is less than 5.5 cm. Ask your doctor to calculate your aortic size index. Because treatment is individualized, it is very important that you see your doctor for an annual CT scan to follow your aneurysm.
For patients with an aortic syndrome, or who are undergoing cardiac surgery for another reason, your surgeon will likely recommend replacing the aorta at a smaller diameter, typically when the diameter reaches 4.5 cm.
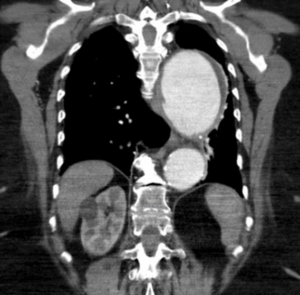
CT scan of a descending thoracic aneurysm. The normal aorta is around 2.5 cm or about the size of a garden hose.
Treatment options for a thoracic aortic aneurysm vary based on size and location within your chest.
These options range from watchful waiting to surgery. If the aneurysm is small and you have no symptoms, your physician may suggest a “watch-and-wait” approach with regularly scheduled images of the aneurysm to check the size. Because aneurysms typically grow very slowly, it is common to monitor them over months or years to determine when the risk of a problem becomes high enough to warrant the consideration of surgery.
Whether your doctor recommends monitoring or surgery, it is very important to keep your blood pressure in a safe range. When your blood pressure is too high, it puts more stress on the wall of the aorta where the aneurysm is located, which can increase the risk of tearing or rupture. Talk to your doctor about your blood pressure and if any medication is recommended to help with this goal. If you are involved in activities or work that might increase your blood pressure significantly like heavy weight-lifting, moving furniture, or extreme stress, be sure to discuss these issues with your doctor to determine any restrictions that may be recommended for your safety. If you are a smoker, you should quit. Your primary care physician can prescribe medications that can help you quit smoking.
If your aneurysm is large enough, or if the aneurysm is growing quicker than usual, surgery may be recommended.
If your aneurysm is detected before it tears or ruptures, surgery would ideally be planned and scheduled with a cardiothoracic surgeon. Be sure to speak with your heart specialist and cardiothoracic surgeon about the risks and benefits of surgery.
Once you decide to move forward with surgery, your cardiothoracic surgeon will recommend replacement or stenting of the affected portion of your aorta with an artificial graft. Not all options are appropriate for every patient, but the surgeons at Newport Cardiac & Thoracic Surgery will talk to you about the recommended operation, including the technique that is chosen and the incision that is made.
A stent placed in the thoracic aorta
If the aneurysm involves the ascending aorta (located in the part of the aorta that exits the heart and travels up toward the neck), the diseased portion can be replaced with a tube graft through an incision on the front of the chest. This incision is called a median sternotomy and extends down the front of your chest, through your breastbone or sternum, which enables your cardiothoracic surgeon to see your heart and aorta.
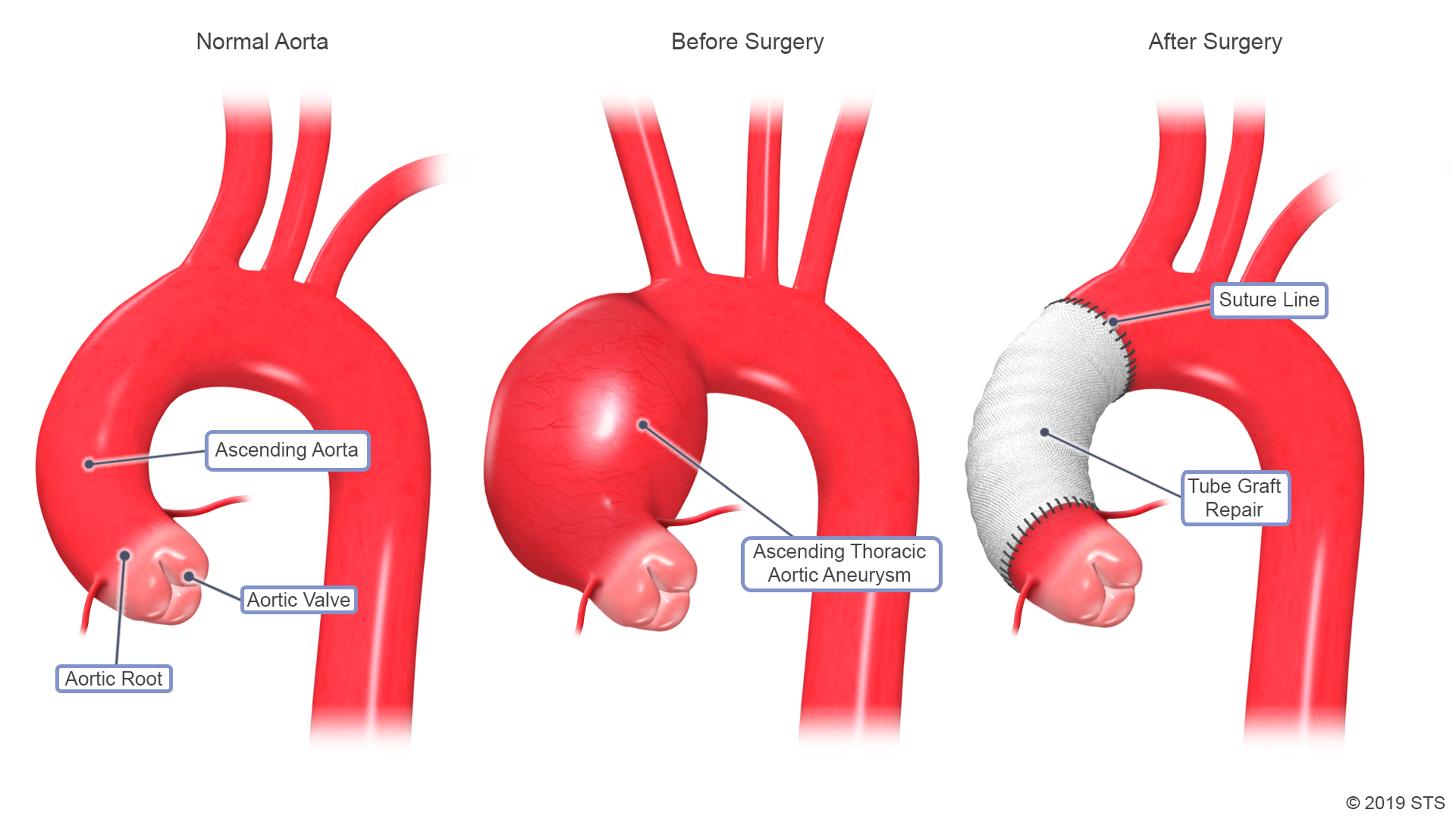
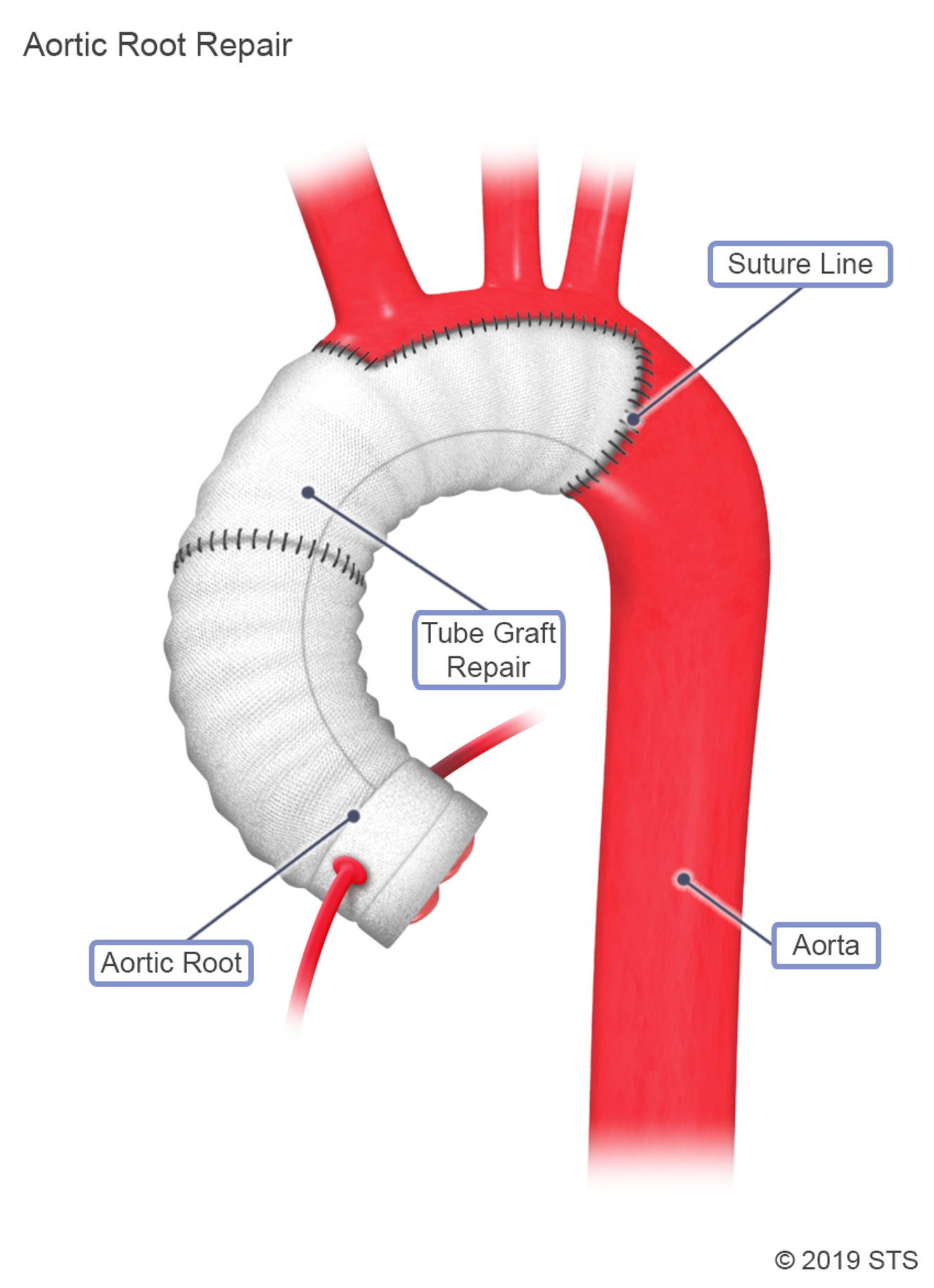
If the aneurysm is close to the aortic valve, the valve also may have to be repaired or replaced. In some cases, the area between the valve and the ascending aorta, called the root, is involved in the aneurysm and will have to be replaced. An aortic root replacement is a more complex operation and your surgeon will discuss the details with you.
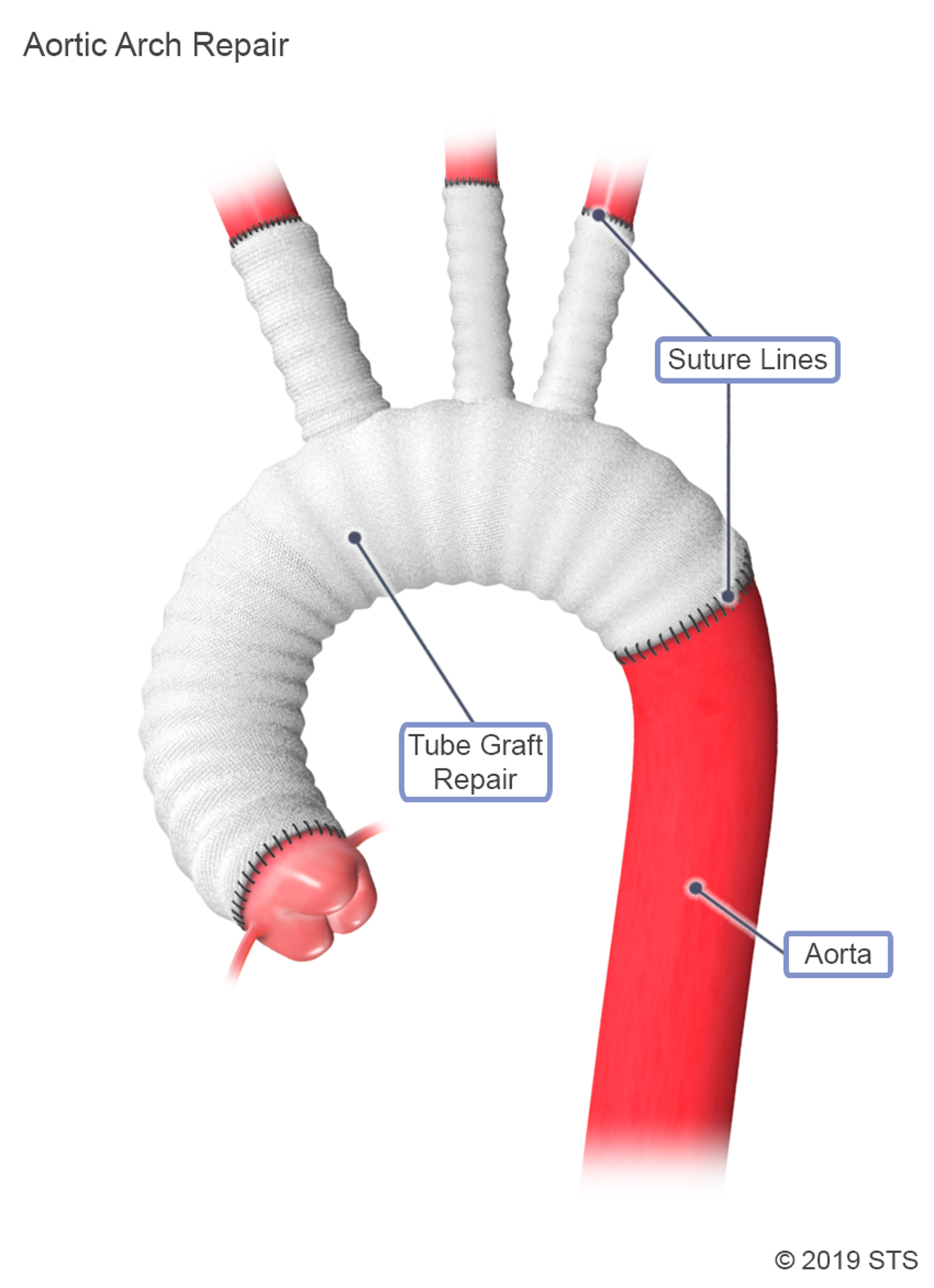
Surgery on the aortic arch (the curve in the aorta that travels up toward the neck, supplying blood to the brain), also is usually done from an incision on the front of the chest. In addition, for the purposes of the heart-lung machine, your surgeon may make an incision near the right collarbone to use the artery that goes to the arm. Because the blood to the brain can be compromised during the surgery, your surgeon will likely take protective measures such as cooling (called hypothermic circulatory arrest). This has shown to decrease the stroke rate associated with this procedure.
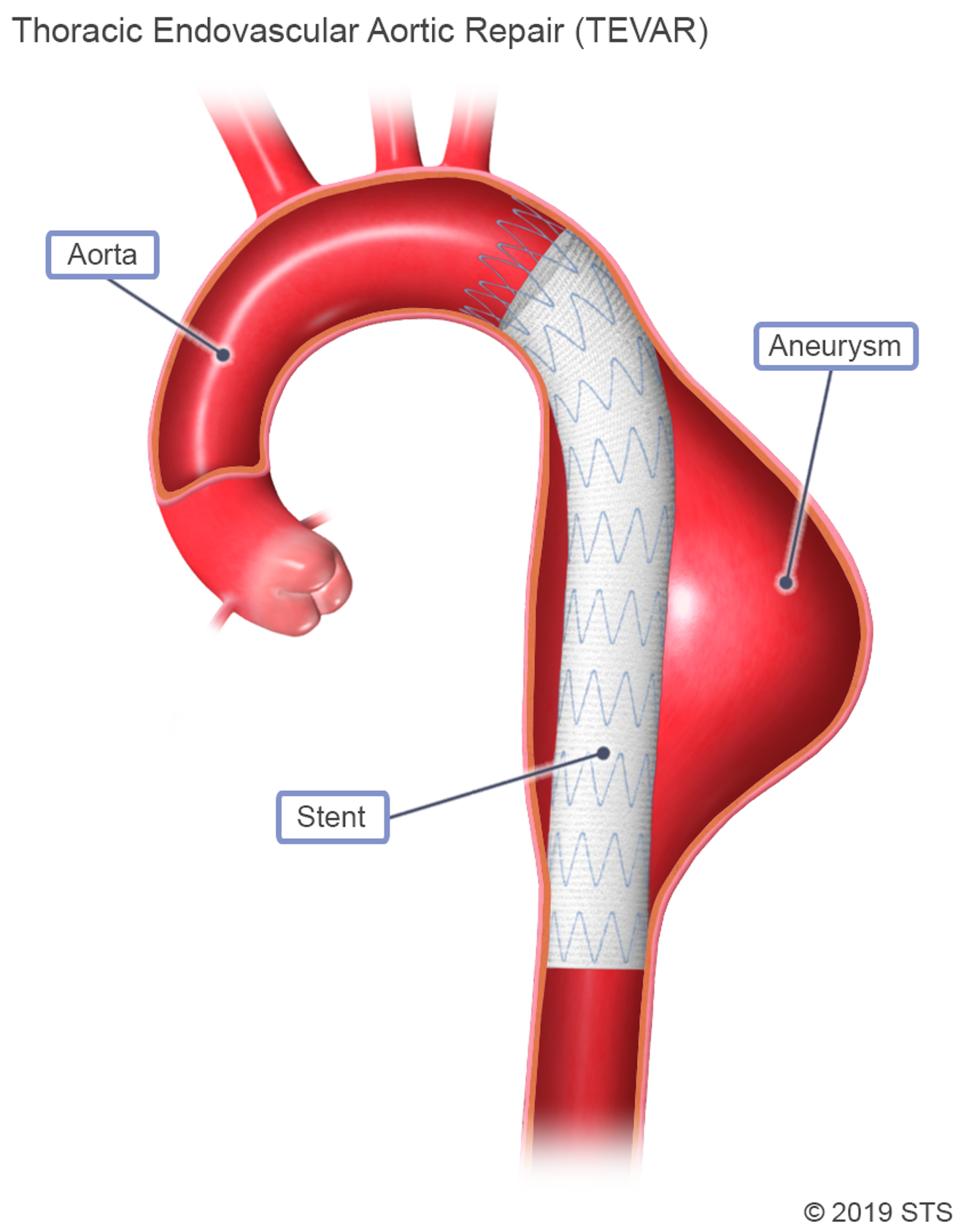
If the aneurysm involves the descending thoracic aorta (the part of the aorta after the curve in the neck which travels down toward the abdomen), a thoracotomy, which requires an incision on the left side of the ribcage, may be required.
Often, aneurysms in the descending thoracic aorta can be treated without an incision in the chest, by relining the aorta with a stent inserted through the artery in the leg. This procedure is called a Thoracic Endovascular Aortic Repair (TEVAR).
The length of the operation and the risks involved depend on the extent of the repair required and on your overall health prior to the operation.
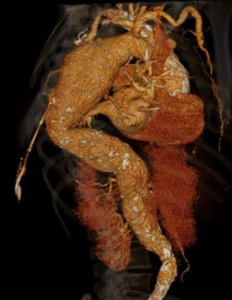
3D CT reconstruction of a descending thoracic aneurysm
When your blood pressure is too high, it puts more stress on the wall of the aorta where the aneurysm is located, which can increase the risk of tearing or rupture.
Recovery
Recovery time following surgery varies based on the size and location of your aneurysm and on the length of your operation. Most people need at least 4 – 6 weeks to recover from the surgery, so you should plan on being out of work for at least a few weeks.
The length of the hospital stay depends on the patient’s condition and the operation performed, but typically patients should expect to stay in the hospital for about a week.
Taking control of your blood pressure and keeping it in a healthy range will help reduce the need for future surgery. You will, however, likely require lifelong monitoring of the diameter of your aorta even after an operation to be sure problems don’t develop in other areas. Keeping regular appointments with a heart specialist will help you monitor your aorta and reduce the chances of future problems.