Aortic Valve Disease
Aortic Valve Disease
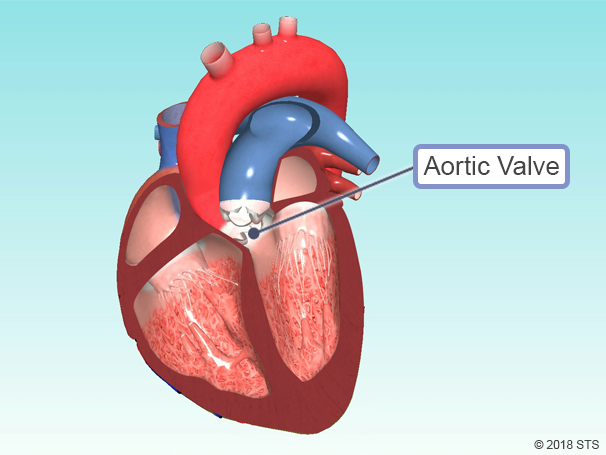
The human heart has four valves—two on the left and two on the right. The aortic valve—the main outflow valve for the left heart—is the valve between the heart and the body. The aortic valve opens when the left ventricle squeezes to pump out blood, and closes in between heart beats to keep blood from going backward into the heart.
Normally, the aortic valve has three flaps (leaflets) that regulate blood flow by opening and closing, allowing blood to flow throughout your body.
Aortic valve disease occurs when the aortic valve doesn’t work properly; it either fails to close tightly (aortic regurgitation or insufficiency) or gets too tight (aortic stenosis).
Types of Aortic Valve Disease

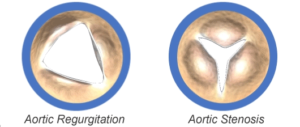
In a healthy aortic valve, valve leaflets open wide to let blood through and close tightly to keep it from going backward. The valve leaflets are thin and pliable.
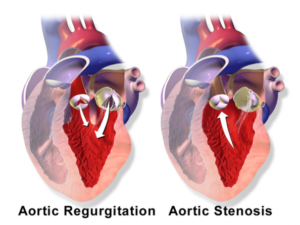
There are two main types of aortic valve disease:
- Aortic Regurgitation (also known as aortic insufficiency) — the valve does not close completely, allowing blood to leak backward into the heart
- Aortic Regurgitation (also known as aortic insufficiency) — the valve does not close completely, allowing blood to leak backward into the heart
Causes And Symptoms
- Shortness Of Breath
- Chest Pain
- Dizziness
The aortic valve may be abnormal from birth (congenital), or it could become diseased with age (acquired).
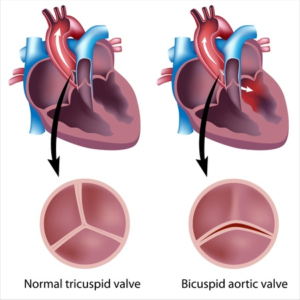
The most common congenital aortic valve abnormality, called a bicuspid aortic valve, occurs when the valve has only two leaflets (bicuspid) instead of three (tricuspid). This prevents the valve from opening or closing completely. Although the abnormality has been there since birth, symptoms may not be felt until adulthood. Your physician may be able to hear distinctive murmurs (abnormal sounds that can be heard with a stethoscope) when listening to your heart.
Acquired aortic valve disease occurs because your valve simply wears out over time, and usually happens as you age. Calcium collects on the valve and can cause the leaflets to stiffen and narrow, which limits their motion.
If the aorta—the main blood vessel coming out of the heart—is diseased, this also can lead to problems with the aortic valve.
A faulty or failing aortic valve may cause symptoms such as shortness of breath, chest pain, and dizziness or loss of consciousness (passing out). These symptoms are due to the heart having to work harder because of the narrowed or leaky valve.
Early on, these symptoms may be noticeable only when exercising, but as the disease progresses, you could experience shortness of breath with minimal or no activity.
Some patients will be unable to sleep flat in bed or may awaken short of breath. Another potential symptom is swollen feet, particularly in the late afternoon or early evening.
Your doctor can usually diagnose aortic valve disease based on your medical history, risk factors, a physical exam, and with results from tests and procedures.
Diagnosis And Treatment Options
There is no one test that can diagnose aortic valve disease, so your doctor may recommend one or more of the following: electrocardiogram (EKG), echocardiogram (echo), chest x-ray, blood tests, and coronary angiography.
Currently, NO MEDICATION can cure aortic valve disease, so it is most commonly treated with surgery.
Aortic stenosis can only be treated with aortic valve replacement. Sometimes, aortic valves that are leaking (regurgitant) can be repaired. Your Heart Team—you, your medical team, and your cardiothoracic surgeon—will determine the best treatment option for you based on your symptoms and test results.
You also can access the STS Risk Calculator, which can help calculate your risk of death or other complications from open heart surgery. The results can help you and your doctor to determine the best course of treatment.
SURGICAL TREATMENT OPTIONS FOR AORTIC VALVE DISEASE
Surgical Aortic Valve Replacement
Surgical aortic valve replacement (SAVR), performed by a cardiothoracic surgeon, involves making an incision in the chest in order to get to the heart and aortic valve. The heart is stopped, during which time the blood pressure and oxygen levels are maintained with a heart-lung machine (cardiopulmonary bypass). The aorta is opened and the diseased valve removed. It is then replaced with an artificial valve (prosthesis).
There are two valve options for aortic valve replacement (AVR) – mechanical valves (metal) or biological valves (tissue).
The principal advantage of mechanical valves is durability—they tend to last your lifetime. However, blood clots can form on mechanical valves, which can lead to stroke, so patients must take blood thinning medication (anticoagulants) for the rest of their lives. Being on blood thinners has a risk of bleeding and patients will have to have their blood levels checked regularly.
Biological valves are most commonly made from animal tissue. Tissue valves are less likely to cause blood clots, and do not require lifelong anticoagulants. However, they are less durable than mechanical valves and may need to be replaced during a patient’s lifetime.
Your Heart Team will discuss with you the advantages and disadvantages of both valve types. Regardless of which valve you choose, there are two different surgical approaches that can be utilized: traditional AVR or minimally invasive.
During traditional AVR, the cardiothoracic surgeon makes a 6- to 8-inch incision down the center of your breastbone (sternum) to open the chest, providing direct access to your heart. In minimally invasive AVR surgery, the cardiothoracic surgeon makes a 2- to 4-inch incision in the top of your breastbone or between the upper ribs on the right side of the chest. The actual valve replacement surgery is the same from either the traditional or minimally invasive approach, but the less invasive option can potentially reduce hospital stay and your pain.


Transcatheter Aortic Valve Replacement
Transcatheter aortic valve replacement (TAVR) is a form of minimally invasive surgery that does not require opening the breastbone. It is used to treat aortic stenosis, and is also referred to as transcatheter aortic valve implantation (TAVI).
Surgeons initially used TAVR when traditional AVR presented too many risks. For example, TAVR was considered if you had been diagnosed with advanced heart, lung, liver, or kidney disease. Now, TAVR can be used to treat aortic stenosis in intermediate and high-risk patients. It is important to know that not every patient is a candidate for this procedure, so talk with your surgeon to decide what treatment option is safest for you.
During TAVR, your surgeon will access the diseased valve through a blood vessel (artery) in your leg (transfemoral). A wire will be threaded back to your heart under x-ray (fluoroscopy) guidance. A hollow tube (catheter) is inserted into your artery through the access point, and a new valve will be placed inside your diseased valve. The old valve is pushed out of the way and the new valve acts like a stent to keep the old valve open.
If the arteries in your legs are not big enough for the catheter and device, your surgeon will discuss other access options. The aortic valve also can be reached from the artery to the arm (subclavian) or the vessel taking blood to the brain (carotid). There are also surgical techniques via a small incision in the breastbone or in the left chest that can be considered.
Two types of TAVR valves currently are available in the United States—one that must be expanded by a balloon and another made of memory metal that self-expands. Your surgeon and the Heart Team will determine which style of valve is best for your anatomy.
Because not all patients are eligible for TAVR, be sure to speak with your doctor about what form of treatment is best for you.
![]()
![]()
Aortic Valve Repair
While the aortic valve is usually replaced, repair may be an option in certain cases, including:
Bicuspid aortic valve repair — The aortic valve leaflets may be reshaped to allow the valve to open and close more completely. This procedure can be used to treat leaking valves (aortic regurgitation), but it cannot be used to treat aortic stenosis.
Repair of valve tears or holes — Tears or holes on the valve leaflets can be patched with a patient’s own tissue.
Recovery
Most aortic valve surgeries have a very low rate of complications; however, potential complications of all surgical options include bleeding, infection, irregular heart rhythm, need for a pacemaker, stroke, heart attack, or death.
Immediately after AVR surgery, you likely will have a tube in your throat so your breathing can be assisted by a ventilator.
The tube will be removed once you are able to breathe on your own. This usually happens within a few hours, but your cardiothoracic surgeon and Heart Team will determine when it is safe. You should anticipate spending several days, but likely not more than a week, recovering in the hospital, although the total length of time depends on your overall health, as well as the specific procedure you underwent.
Once you’re home, it may be several more weeks until you are able to go back to work. Everyday activities such as driving and lifting heavy objects may be restricted for a period of time. Typically, lifting and activity restrictions are 4-6 weeks for traditional AVR and 1-2 weeks for TAVR.
Blood thinning medication may be prescribed after surgery, but your need for this medication will be determined by your doctor.
After your wounds have healed, you should be able to get back to your normal activities. Always tell a doctor about your valve surgery before any medical procedure. In particular, you may require preventative antibiotics when having dental work.