What Is ECMO? Extracorporeal membrane oxygenation (ECMO) is a technique that replaces the functions of failing lungs and/or the heart.
People with life-threatening but reversible heart or lung illnesses who have not responded to standard treatments may be candidates for ECMO. For example, ECMO may be used for severe lung damage from infection or shock after a massive heart attack. ECMO also can be used to support a failing heart after heart surgery. ECMO can provide support for days to weeks while doctors treat the underlying illness.
Extracorporeal means that the blood circulates outside of the body through a tube or catheter with the help of a machine. Membrane oxygenation, referred to as the “artificial lungs,” is a special part of the machine that puts oxygen into the blood and takes out carbon dioxide, just like the lungs do. ECMO also is known as extracorporeal life support (ECLS), and the ECMO machine often is referred to as a type of heart-lung machine.
During ECMO treatment, the heart continues to beat, but its work is made easier because the ECMO machine does much of the pumping. The goal of ECMO is to ensure that the body has enough blood flow and oxygen by temporarily managing the workload of the heart and lungs. ECMO provides time for the body to rest and recover, but it will not directly heal the heart or lungs.
ECMO was initially developed and used for babies in critical condition whose lungs were not functioning, but it is now being used more for adults. According to the Extracorporeal Life Support Organization (ELSO), more than 100,000 patients have been on ECMO over the past several decades.
Being placed on ECMO requires a surgical procedure to insert catheters or special tubes, known as cannulae, into the veins and arteries. This is usually performed in the intensive care unit or the operating room. It’s important to know that ECMO support is generally not painful.
The patient will be sedated, as well as given pain medication and an anticoagulant to minimize blood clotting. A cardiothoracic surgeon, assisted by an operating room team, will insert the cannula into the neck, groin, or chest, while a specially trained respiratory therapist prepares the ECMO machine. The number of tubes placed will depend on how ECMO is being used. Physicians and nurses from the intensive care unit (ICU) will closely monitor the patient during the procedure and make sure that he/she remains stable and comfortable.
An x-ray is taken to ensure that the tubes have been placed correctly. Once the cannulae are properly inserted and secured, the ECMO machine is connected and the pump is started. Routine monitoring equipment will measure the heart rate, respiratory rate, oxygen levels, and blood pressure. A breathing tube that is attached to a ventilator will be inserted through the patient’s nose or mouth. This is needed to prevent the lungs from collapsing while they heal. Intravenous catheters also will be connected to tubes that provide continuous administration of medications. The ECMO pump and circuit will be located next to the bed.
Since ECMO is used in very serious cases, the patient may already be sedated when placed on ECMO. Additional medicine may be administered to keep the patient asleep until he/she is weaned off of the ECMO machine. If the patient is sedated and has a breathing tube in place, supplemental nutrition will be provided either intravenously or through a nasal-gastric tube. However, it’s also possible that at some point, the patient may be awake and able to interact with people. He/she may even be able to walk.
The length of time the patient remains on ECMO depends on the diagnosis and individual response.
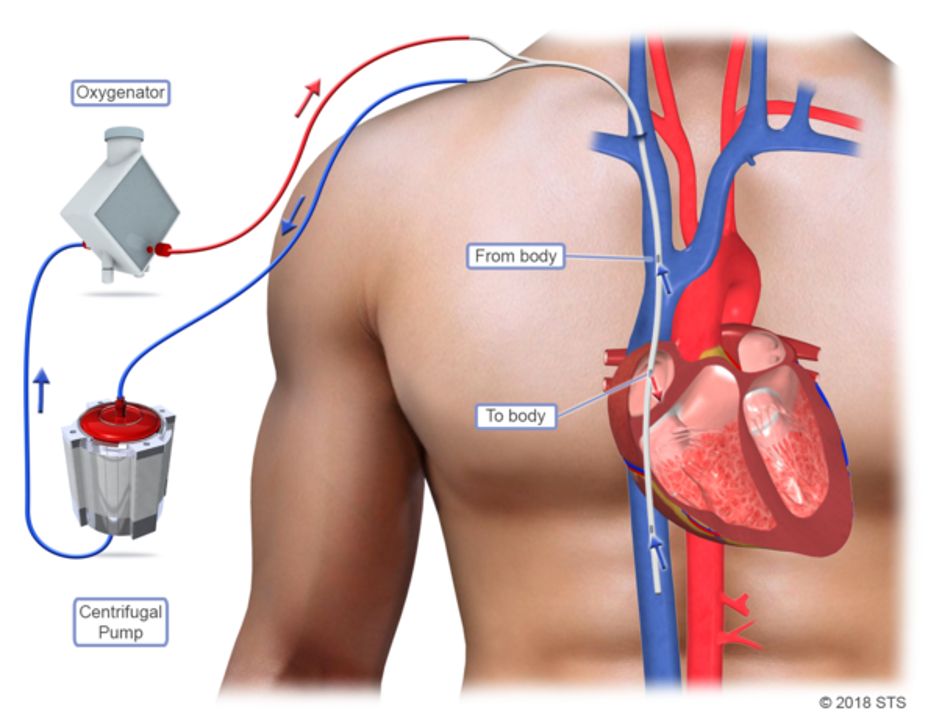
The ECMO machine has many connecting pieces and moving parts. It consists primarily of a pump and a circuit made up of a membrane (artificial lung), a blood warmer, and a filter. The machine removes blood without oxygen and pumps it through the membrane where carbon dioxide is removed and oxygen is added. The oxygenated blood is then warmed to body temperature, filtered, and returned to the body. The ECMO specialist adjusts the amount of flow to meet the patient’s requirements. As the heart and/or lung function improves, the flow is decreased.
The two most common types of ECMO are veno-arterial ECMO (VA ECMO) and veno-venous ECMO (VV ECMO). The ECMO team will decide which type will help the patient the most, based on his/her specific illness.
The VV ECMO machine is connected to one or more veins, usually near the heart, and is used to support only the lungs. Based on the patient’s age and condition, the cardiothoracic surgeon may choose to place one special cannula in a single vein that is close to or inside the heart or two cannulae in different veins.
The special cannula in one vein has two channels, side by side inside the tubing, allowing the ECMO pump to draw blood out through one channel and back in through the other. In this case, there is only one entry site instead of two.
The ECMO machine will remove un-oxygenated blood from the vein through the cannula, add oxygen to the blood, remove carbon dioxide, warm the blood, and return the blood to the heart. At that point, the heart takes over and pumps the oxygenated blood throughout the body, so that the lungs have time to rest and recover.
In VV ECMO, no cardiac support is provided.
ECMO is used for infants, children, and adult patients who have illnesses in the heart or lungs and who are not able to supply oxygen to their own bodies. It is important to understand that anyone who needs ECMO is critically ill.
Patients’ lungs fail for a number of reasons, including pneumonia, lung cancer, pulmonary edema, pulmonary embolism, and chronic obstructive pulmonary disease (COPD). When the lungs fail, the patient will first be intubated (breathing tube) and hooked up to a ventilator (breathing machine). However, sometimes lungs are so damaged that providing oxygen through intubation is not enough. This is usually when doctors determine that VV ECMO is necessary. A heart can fail for many reasons, including heart attack, pulmonary embolism, bad valve disease, or worsening heart failure. When a heart weakens, doctors try to fix the underlying problem, sometimes with medications to help improve the pumping function of the heart. If medications do not work, doctors will use VA ECMO.
ECMO also is used for older children suffering from postoperative cardiac repair, trauma and other emergencies, pneumonia, asthma, congenital heart defects, and aspiration of toxic materials into the lungs (lighter fluid, turpentine).
While on ECMO, the patient will be monitored constantly and very closely by an ECMO team that consists of specially trained professionals devoted to his/her care. The team may include:
Cardiothoracic surgeon – places the cannulas needed for ECMO
ECMO physician – directs ECMO treatment from start to finish
Interventional cardiologist – also performs ECMO placement
Vascular surgeon – removes the cannulas needed for ECMO
Perfusionist – has specialized training and certification in running the ECMO machine
ECMO coordinator – prepares the ECMO machine and tubing and troubleshoots any problems
ECMO specialist – manages the ECMO circuit and its effect on the patient
ICU nurse – monitors the patient, administers medications, and provides the patient with any other care he/she may need
Respiratory therapist – provides breathing treatments and helps manage the breathing machine
Other team members who may be involved include a dietitian, physical therapist, social worker, and chaplain, as well as a kidney doctor and nurses.
The ECMO team will take daily x-rays to make sure the tubes are in the right place and to see if the patient’s lungs are looking better. Blood samples also are tested for improvements. In addition, the team will keep an eye on the heart rate, respiratory rate, oxygen levels, and blood pressure.
The ECMO physician may want to perform a bronchoscopy to look inside the lungs and see how they are healing. This procedure involves threading a small, flexible bronchoscope tube, with its light and small camera, through the nose or mouth, down the throat into the trachea, or windpipe, and through the airways in each lung, checking for problems. In addition, it is likely that the patient will have regular neurologic exams to ensure that he/she is receiving enough oxygen delivery to the brain. The arms and legs also will be examined to make sure oxygen is traveling to all four limbs and that there have been no complications.
While on ECMO, the breathing tube and ventilator will keep the lungs working and help remove secretions, while medications will transfer continuously through intravenous catheters. The patient may receive certain medications, such as:
If the ECMO team thinks that the patient may be improving, they may decrease some of the medications supporting the heart and lungs, or turn down the pump flow. This allows the team to determine whether the heart and lungs can do more of the work on their own. The function of the heart and lungs are measured by blood samples, chest x-rays, chest movement, and echocardiogram.
If the test results look good, the ECMO team will discuss removing ECMO, often called a “trial off.” The ECMO team will decrease support and/or take away ECMO for minutes or hours to see if the patient needs to stay on ECMO. If the trial shows that he/she needs more time on ECMO, the patient will be put back on support. If during this time, he/she remains stable, ECMO can be discontinued.
If the patient is ready to come off ECMO, the cardiothoracic surgeon will remove the cannulae. If the cannulae were placed through the skin without a large incision, they will be taken out like an IV with firm pressure. If the cannulae were surgically placed (through an open incision), they will be surgically removed and the vessel will be repaired with small stitches. This can be done either at the bedside or in the operating room. The patient will be asleep and monitored during this process.
The breathing tube and ventilator may still be needed, but will be decreased as the patient improves over time. A physical therapist and rehabilitation specialist will work with him/her to regain strength. It is a slow process, but the patient can expect to get stronger each day.
The patient can stay on ECMO anywhere from 3 days to a month. The longer he/she remains on ECMO, the higher the risk of complications
While ECMO can be potentially life-saving, there are risks and complications associated with its use. The ECMO team will discuss these details with the patient and/or the caregivers before placing the patient on ECMO. The ECMO specialist and ICU nurse are specially trained to handle any problems that happen with the ECMO machine. In addition, it is possible that the patient may need to temporarily come off the ECMO machine in order to fix a problem. During this time, he/she will receive the necessary support. In most cases, the ECMO machine can be repaired or replaced and ECMO support restarted.
The most common complication is bleeding. While heparin, an anticoagulant medication, reduces the formation of clots within the ECMO machine, it also reduces the patient’s ability to clot. As a result, he/she is at increased risk for bleeding at the surgical sites, internal bleeding, and bleeding in the brain. The ECMO team will run labs often and will carefully adjust the amount of heparin. Ultrasounds also may be used to look for bleeding, in addition to the ECMO team watching very carefully for changes in how the patient acts and his/her ability to do certain things like squeezing a hand or wiggling the toes.
Whenever a large tube is inserted in veins or arteries, there is an increased risk of surgical complications, stroke, and infection (especially at the sites where the cannulae are placed). In addition, small blood clots and air bubbles can sometimes appear inside the ECMO tubing. The ECMO team will conduct many tests to help them recognize any of these problems.
Other complications include:
If any problems occur, the ECMO team will speak with the patient and/or the caregiver in an effort to fix the issue as soon as possible and to decrease further risks.
It is important for a patient to talk to his/her family members and doctors about what he/she would like to happen in different situations. The more clearly the patient explains his/her choices to loved ones and health care providers, the better they will be able to follow the patient’s wishes if he/she is unable to make decisions for him/herself.
{kind=link}
{kind=link}