Barrett’s Esophagus
Barrett’s Esophagus
The esophagus (ĕ-sof´ah-gus) is the hollow, muscular tube that moves food and liquid from your mouth to your stomach. A ring of muscle fibers at the bottom of the esophagus keeps the stomach contents from moving backward.
In some people, the muscles of the esophagus don’t work properly so the contents of their stomach flow backward into their esophagus on a regular basis (chronic acid reflux). Barrett’s esophagus can occur when the reflux continually damages the lining of your esophagus.
No one knows how many people have Barrett’s esophagus, but it is estimated to affect one in every 15 people. The National Institute of Diabetes and Digestive and Kidney Diseases reports that Barrett’s esophagus occurs twice as often in men than in women and more often among Caucasians than any other race.
Causes Of Barrett’s Esophagus
Many doctors agree that the main cause of Barrett’s esophagus is recurring reflux of acid or other stomach contents into the esophagus, which damages the esophageal lining.
It is also thought that some people are predisposed to developing Barrett’s esophagus based on their genetic makeup.
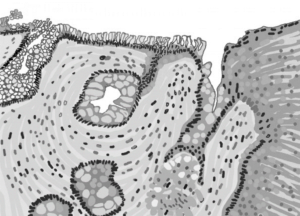
Drawing of a microscopic piece of the esophagus showing the abnormal tissue of Barrett’s esophagus.
Symptoms Of Barrett’s Esophagus
- Heartburn
- Reflux
- Dyspepsia
Barrett’s esophagus usually does not cause any signs or symptoms, but there is a strong relationship to long-term gastroesophageal reflux disease (GERD). Symptoms of Barrett’s esophagus may be similar to those of GERD:
- A burning sensation in the chest (heartburn)
- Backing up of stomach acids (reflux) with a sour or bitter taste in your mouth
- Stomach discomfort (dyspepsia) with nausea or bloating after eating
If you have a history of heartburn or acid reflux or have been diagnosed with GERD, ask your doctor about your risk of developing Barrett’s esophagus.
People with Barrett’s esophagus have a higher risk of developing esophageal cancer.
Diagnosis And Treatment Options
The only way to diagnose Barrett’s esophagus is with an upper endoscopy and biopsy. During an endoscopy a long flexible tube with a camera is placed through your mouth into your esophagus. You will be given a sedative before the procedure, so it may feel uncomfortable but will not be painful.

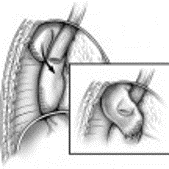
Endoscopic view of Barrett’s esophagus
If your esophagus shows signs of damage, your doctor will remove a small sample of tissue (biopsy) that will be examined under a microscope to confirm a diagnosis. The biopsy also will be used to check for signs of cancer or precancerous changes (dysplasia).
If the biopsy confirms the presence of Barrett’s esophagus without the presence of precancerous cells, your doctor likely will recommend that you have periodic repeat endoscopies to continually monitor for any signs of esophageal cancer. This is done as a precaution because cancer can develop years after diagnosing Barrett’s esophagus.
No medications can reverse Barrett’s esophagus, but there are things you can do to improve acid reflux symptoms and slow the development of Barrett’s esophagus. Your treatment will vary depending on whether your doctor found precancerous or cancerous cells during your biopsy.
If your biopsy did not show cancerous cells, your treatment may consist mainly of lifestyle and diet changes to reduce and control acid reflux, including:
- Limiting fatty and spicy foods, chocolate, and caffeine
- Reducing intake of alcohol
- Avoiding tobacco use
- Losing weight
Your doctor also may prescribe medications to reduce the amount of acid your stomach produces (proton pump inhibitors) or recommend antacids after meals and at bedtime.
If cancerous cells were found in your biopsy, various treatment options are available, including the surgical removal of your esophagus (esophagectomy).
Surgery may not be an option for some people, so if your doctor or cardiothoracic surgeon think surgery is not right for you, other treatment options are available as outlined below.
Antireflux Surgery
Patients with Barrett’s often have a hiatal hernia (the stomach has pushed up through the diaphragm and into the chest), which can be repaired laparoscopically or robotically during antireflux surgery, although a larger incision through the chest or abdomen may be recommended, especially if your hernia is larger, you are overweight, or your esophagus is relatively short due to scarring.
Options for antireflux surgery include Nissen fundoplication, LINX magnetic sphincter augmentation and transoral incisionless fundoplication (TIF).
During Nissen fundoplication surgery, the upper part of the stomach (fundus) is wrapped around the esophagus to reinforce the valve between the esophagus and stomach, making acid less likely to back up into the esophagus. The procedure usually is done using a minimally invasive (laparoscopic) approach through small incisions in the abdomen.
LINX magnetic sphincter augmentation consists of an implantable magnetic band surgically placed around the lower esophagus.
Transoral incisionless fundoplication (TIF) is an endoscopic procedure performed by a surgeon or highly specialized gastroenterologist. If the patient has a hiatal hernia a surgeon will need to reduce and repair the hernia, usually performed with minimally invasive robotic surgery, in combination with TIF.

Endoscopic Mucosal Resection
Uses an endoscope to remove superficial abnormalities (Barrett’s esophagus, dysplasia, and very early cancers) limited to the inner lining of the esophagus (mucosa)
Radiofrequency Ablation
Uses heat to destroy abnormal esophageal tissue (Barrett’s esophagus as long as there is no suspicion of dysplasia or cancer); may be recommended after endoscopic resection


Cryotherapy
Uses an endoscope to apply a cold liquid or gas to abnormal cells in the esophagus. The cells are allowed to warm up and then are frozen again. The cycle of freezing and thawing damages the abnormal cells.

No medications can reverse Barrett’s esophagus, but there are things you can do to improve acid reflux symptoms and slow the development of Barrett’s esophagus, including: limiting fatty and spicy foods, reducing consumption of alcohol, avoiding tobacco use, and losing weight
Recovery
Most endoscopic treatments are performed as an outpatient (a patient who receives treatment but is not hospitalized overnight). Laparoscopic antireflux surgery usually requires a 1-2 night hospital stay with full recovery in 3-4 weeks.
If you undergo an esophagectomy, you should expect to spend approximately 7 days in the hospital. You should expect recovery to take about 6 to 8 weeks. Most patients eventually return to normal activities. If your job requires heavy lifting, your doctor may recommend that you take about 3 months off work following surgery; however, if your job is less strenuous, you may be able to go back to work in about 6 to 8 weeks. Be sure to discuss your specific recovery with your doctor before the surgery, and at any follow-up appointments
You also will need to adjust your eating after the surgery. Most patients benefit from eating smaller, more frequent meals after esophagectomy because you tend to feel full very quickly.
Patients also should avoid eating for 3 hours before sleeping and should sleep at a 30° angle using pillows or a foam wedge to help prevent stomach contents from coming up and getting into the lungs.
Some patients may experience nausea, vomiting, cramping, flushing (blushing; redness of the skin), or diarrhea when their stomachs become overly full (distended); limiting liquids with your meals may help reduce these symptoms. Sweets, such as candy, sugar, syrups, and honey also may contribute to this problem. If you experience any problems while eating, speak with your doctor.
People with Barrett’s esophagus also have an increased risk of developing esophageal cancer.
Although the risk is small, it is important to have regular checkups with your doctor to monitor your condition.